It’s been half a year since I’ve posted here. I hope you didn’t miss me too much. I’ve been busy living.
I write today to commemorate the 6th anniversary of my stem cell transplant. I distinctly remember that six years and a few months ago I was struggling with thoughts of what lay ahead. I knew that a transplant was my best hope of achieving a meaningful reversal of the myeloma that invaded my blood. Still, the many risks, and stories of horrendous side effects, left me wary. I was ready but frightened.
As it turned out, the transplant and my recovery went smoothly. I was home in about 30 days and I showed no signs of myeloma in regular blood tests about six months after the transplant. A few years later I tested MRD negative. At the time of the transplant, I hoped I would achieve at least two or three years of minimal disease involvement before I might need major treatment again. Here I am, six years later. Happy, healthy, and looking at life’s future.
I’m not superstitious or one to think I may jinx myself by writing these words, but you’ll excuse me a moment while I knock on some wood. I haven’t written here lately because I’ve been busy living. We are working around the house, planting, decorating, and remodeling. I’ve been snuggling my newest granddaughter and watching the others grow big. I’m witnessing my own children become amazing adults. I started down new career paths and I’m looking at other changes before retirement. All this living, without concern that my myeloma may return.
Isn’t that the goal for all of us? To live every day to the fullest without concern it will end one day. With my cancer diagnosis seven years ago it felt like I was being shown the when and how of my demise. I was merely marking time for the inevitable. Now I know that isn’t true. Will my myeloma return soon. That is possible. Will I ultimately leave this earth earlier than I’d hope? Isn’t it always “earlier” than we’d hope?
My diagnosis plays a part of my life every day. I take a fist full of medications every morning and night, one of which specifically targets the myeloma. I get blood drawn every two months and visit my doctors to review the results. I’ve had extra boosters and vaccinations to help avoid a serious case of Covid-19 or other diseases. Myeloma is inextricably connected to my day-to-day life. Even so, I’ve reclaimed control of my life from the disease.
I know not all myeloma patients are as fortunate in their treatment as I have been. I also know many patients like me live full lives beyond their diagnosis. Seven years ago I learned I had a “high risk” variant of incurable cancer and my life may be cut short. I was told and wanted to believe that statistics are meaningless in real life. The only statistic that matters to your disease is what happens to you. Will I respond well to treatment? Will I achieve many healthy post-transplant years?
While the answer to these questions can be different for every patient, I’m here to say it can happen. It happened to me. Looking forward from diagnosis is such a difficult and frightening task. Looking back from an undetermined but hopeful future is a luxury.
I will try to share more of my experiences as a myeloma patient here, but you’ll excuse me it I keep busy with all the other glorious parts of living.
For a child, five years can be a lifetime. They grow so big, they learn so much, and they experience so many new things. For adults that same amount of time flashes past in a blink, often without much change. When you undergo a stem cell transplant they sometimes call it your “re-birthday.” My re-birthday was five years ago, and like a child, it seems like a lifetime has passed since July 22, 2016.
When I was diagnosed a year before my transplant I wasn’t suffering much physical illness. I was one of the lucky myeloma patients that discovered the disease during a routine blood test before it had a chance to do much damage to my body. At the time fear and anxiety became my biggest ailment.
During an early conversation with my doctor, I was told I might only survive six years. When I heard those words I understood very little about myeloma or its treatment. The thought of not surviving to my 60th birthday often paralyzed me. Strong support from loved ones, professional counseling, education, and time allowed me to move well past the debilitating shock I suffered.
The other memory that seems so far away today is of the many hours spent driving to the cancer clinic, sitting in waiting rooms, and enduring tests and procedures. The early days of testing and treatment were scary. While it became somewhat “routine” over time it was never normal. For now, thankfully, that part of this new life is on hold.
I was lucky to experience a relatively easy transplant, but looking back, I have perspective on the impact even that “easy” transplant had on me. In the first year following transplant I was definitely in “recovery” mode. I spent a frightening night in the ER with an unexplained 102 fever. I suffered frequent coughs and colds, many times requiring trips to the walk-in for chest x-rays and medications. Fatigue was a real thing and naps were frequent. My muscles were far weaker than my pre-transplant non-athletic form. Over time, however, most of these reminders of my cancer have faded.
At the beginning of 2020, I learned all the hard work paid off. Tests revealed that I was MRD negative. The most sophisticated testing science currently offers detected no myeloma cells in my body. While regular blood tests were clear for over a year, the MRD test was monumental. The test confirmed that myeloma isn’t lurking behind the stable blood tests and my general good health.
2020 was historic for the world, not just me. Like so many, when I left the office in March and began working from home there was no way I thought I would still be here over a year later. The uncertainty surrounding the virus, and its deadly consequences put most people on edge. Having a compromised immune system, which appeared to be working very well, caused me concern. I certainly paid more attention to the health warnings and followed the most conservative advice. Eventually, my wife and I settled into our covid inspired home office and reinstated our transplant cleaning protocols to stay safe.
Given how strange life was for everyone last year, I’m hard-pressed to feel I was any more impacted than the majority of people. Being separated from people probably contributed to the fact 2020 was the first year since my transplant I didn’t have at least one cold or coughing spell. With the amazing introduction of multiple effective vaccines, there is hope we will all return to “normal” very soon. On this anniversary of my re-birth, the world is showing encouraging signs of its own reincarnation.
I’ve passed the initial six-year prognosis; in fairness, my doctor was optimistic I would beat that number. I’ll be celebrating my 60th birthday later this year. I remain cancer-free, my test results are stable, and I feel healthy. The aches and pains I complain about now appear more associated with being 59 than being a cancer survivor.
Since my cancer diagnosis and transplant my life has changed so much, and for the better, in these five years. My grandchildren are growing and another will join us in November. My adult children are living incredible lives. My wife and I inch closer to our retirement plans. Contrary to ending my career I’m pursuing exciting new opportunities. Most significantly, with a better understanding of myeloma, the success of my current treatments, and the development of even more treatment options, I’m hopeful that I will continue to enjoy many more cancer-free days.
For over 30 years our house has been the home of Thanksgiving. When we were college students our apartment was the place students who couldn’t make it home for the holidays would convene. When we moved back to Washington, family, friends, friends-of-family, new significant others, new babies, and new pets migrated yearly to our home to celebrate. We will miss that this year.
Our circumstances are not unique as families across the country will experience Thanksgiving differently this year. If your traditions involve gathering with friends and family, eating, watching football, playing games, chatting, arguing, and giving thanks, this year will be strange. Granted, not everyone will heed the medical cautions and congregate as usual. I pray they don’t pay a terrible price.
Thanksgiving is my favorite holiday. There is no contest. While there are traditional foods to enjoy, my primary joy comes from the gathering. I’m close with my family, we stay in touch throughout the year, but this is the time we are all together. There is an indescribable connection on this day. Memories of Thanksgivings past and family that are no longer with us are shared. We laugh about things that happened years ago and five minutes ago. Oh, how we laugh.
I remember the first Thanksgiving after my diagnosis. While myeloma has never put me on death’s door, I’ve contemplated my early departure and how precious these times are. I’m fighting not to feel cheated this year since my health is so good. How many more Thanksgivings will I be given? While I know these negative thoughts are unhealthy I feel a greater loss this year because I know how valuable my limited time with family is.
I must pack my depressing thoughts away and deal with the hand that was dealt. That’s not denial, but acknowledging what is. The warnings are real and they are clear. We can’t safely gather this year as we have in the past. Mourning that loss, or projecting to an unknown future is pointless. I can, however, be happy for what I have. I have a choice to keep my family safe and I have hope for a better tomorrow.
There will be over 250,000 empty chairs at Thanksgiving celebrations this year. The families and friends of those lost to Covid don’t get to decide if it might be safe to get together. They don’t get to bring the family together and hope the virus skips their holiday table. For the loved ones of the passed the holidays will never be the same.
I will stay the course on my treatments and I have faith my myeloma journey has miles to go. I will be able to hold my family again and share their love. Whether it is Thanksgiving 2021 or some other day, we will be together again. In 2020, for everyone’s safety, we won’t gather on the fourth Thursday of November. Perhaps it will happen in June of 2021. Does it matter on which day we join again? If we stay safe today, we will have a tomorrow to join again.
This year we will spend the holiday Together, Apart.
In 2015 I thought my cancer diagnosis would be the scariest thing that would happen the rest of my life, and then came 2020.
I’ve been working from home since March 10, 2020. I haven’t been able to add to this blog since shortly after being ordered to stay home by my doctor, my governor and, my employer. It isn’t that I didn’t have time, or didn’t have thoughts to share, I just found it difficult to translate my feelings into words. It isn’t any easier today, but I’m compelled to try.
As I sit here this morning I’m watching pictures of my city and my country burning. The tally of souls lost to Covid-19 moves past 100,000 with no clear end in sight. The divisions in our communities grow into chasms that may never heal. I am heartbroken and I am scared.
This blog is about my journey with multiple myeloma. It has never been political, even if discussing the U.S. healthcare system sometimes touches on politics. I still don’t intend to be political, but what is happening is so profound, I can’t write about my cancer without acknowledging the world in which I’m trying to survive.
When I was diagnosed with cancer I was scared. First I grieved for myself, thinking about the years I might lose and the things I might miss. I was also sad for my family and loved ones, for leaving them without my support. Those feelings were personal as the world around me kept going. Part of the challenge of survivng with cancer is learning to function in the “normal” world while my existence is threatened. In the last few months, while my disease reached healthy stability, the world around me unraveled. Today I fear for us all.
In my last column I wrote about the need for everyone to understand the threat of infection to those of us in high-risk categories. I was hopeful that people would learn we’re all in this together and those of use with underlying health threats depend on the otherwise healthy population to keep us safe. Sadly, since writing that column I’ve witnessed acts of unbelievable selfishness and ignorance. The death toll from this virus is far beyond what it likely could have been if only we were united in our efforts to defeat it.
As spring moves to summer our leaderships’ focus turns to putting people back to work to get commerce flowing even though all reasonable evidence suggests we are far from through the threat of this pandemic. A lesson I learned after my diagnosis is that no matter how well I respond to treatment I will never return to my pre-diagnosis life. Too many of our population fail to understand the threat of this virus has changed our lives forever. We are not going back to pre-covid lives. We can’t wish away Covid-19 any better than I can wish away my cancer.
As the length of our quarantine stretched into months the news was dominated by images of armed, mostly white, protestors occupying capital buildings demanding states to “reopen”. What we didn’t see were police meeting these heavily armed and agitated protestors with tear gas and rubber bullets. Instead, they were allowed to carry their weapons into the halls of legislation to scream their demands.
The pandemic laid bare the divides in our country. People of color were carrying the burden of keeping our essential services operating and paying the price with their lives in disproportionate numbers. Even though the health threat isn’t over, many in power have calculated this cost of moving the economy forward is acceptable.
In my sadness watching this modern plague ravage our country I was stunned by images of black men murdered in broad daylight by vigilantes and people sworn to protect us. Unfortunately, our history is bloody with these killings, but those murders, in this time, led to protests and violence in the streets across the nation.
People are in the streets demanding justice for all people of color. The crowds are large and diverse and the message is familiar. These crowds, unlike those we saw earlier in the month, are being met by militarized police, tear gas, and rubber bullets. People in leadership, ostensibly condemning the murders are demanding swift retribution for the unruly protests.
I don’t condone violence by anyone, but the response to the two groups of protestors couldn’t be starker or more disturbing. We can only hope the convergence of events will open eyes and hearts.
With or without myeloma, I’m approaching the end of my time on this planet. My generation squandered its chance to make this a better world. I fear what we’ve left for my children and grandchildren.
While today I feel overwhelmed with sadness, I can’t count the number of times in the last three months I’ve been brought to tears witnessing stories of human strength and love. We’ve seen kindness and heroics from people of every color and background. Will the inherent goodness of people someday overcome the systemic evils?
I experienced an unexpected emotional response when I learned I was going to cut back the treatment regimen I’d been on for nearly four years.
It is difficult to describe how surprised I am. I’ve thought about this day a lot. I’ve written about it here more than once. I was disappointed when I thought it wasn’t going to happen. Still, I didn’t expect the deep emotional feeling I experienced as I walked out of the treatment bay for the last time.
Let me back up a minute.
Following my autologous stem cell transplant (ASCT) in 2016, I began an aggressive three-drug maintenance regimen of Kyprolis, Pomalyst, and Dex (KPD). Three years later, in September 2019, I met with my doctors expecting we would reduce the treatment. I was disappointed when he recommended continuing the treatment, but with possibly lower doses.
Not only did I feel disappointed, irrationally perhaps, I also felt defeated. This was a low spot for me emotionally. I wondered if I’d ever feel I’d advanced in my treatment or ever get a break from the constant treatment.
Before making the final decision on the on-going treatment we agreed to undergo more precise testing; MRD testing. I’ve shown no monoclonal proteins in my blood tests in at least 3 years, so is it possible that I have no minimal residual disease? As I just wrote, I underwent a bone marrow biopsy and a PET/CT to confirm that I am MRD-. This is the best possible response a myeloma patient can achieve under today’s testing methods. It is not a cure, but it is a very deep response and a statistically good predictor for a long progression-free survival and longer overall survival.
With that great news, I met again with my doctor and his view had changed. He was ready to recommend Pomolyst only maintenance. No more Carfilzimib and, surprisingly no more Dexamethasone.
I’d given this much thought for months. Even though my gut tells me Carfilzimib may have been the heavy hitter getting me to MRD-, I want to take advantage of this moment of good health, no matter how short, to enjoy my life a bit more. My schedule opens, the treatments are easier, I spend more time at home, and less time driving and sitting in treatment. It is worth the chance that I may open the door to relapse even a crack to get some life back. Of course, we won’t take our eyes off the ball.
I will get blood drawn at a lab near my home once a month. I will see my care team at Seattle Cancer Center every two months. We may do another biopsy and MRD test in a few months to watch for early signs of relapse. Even so, hours, days, weeks of my life will no longer be spent driving to and from Seattle, waiting for labs, and waiting for infusions. I received a great gift of time.
Of course, this is all the cerebral part of the decision to change. I was unprepared for the emotion that was about to sneak up on me following my final carfilzomib infusion.
When I posted a short note about my new treatment plan to a General Myeloma Facebook group, a fellow patient commented, “It’s surreal, too, isn’t it? You may find you seem to have a lot of time on your hands, or you keep feeling like you’ve forgotten something. It’s awesome and terrifying at the same time.” She’s right. Surreal is exactly the feeling that began to wash over me at this moment. I’m also sure there will be days when my body expects to make a trip to Seattle and I’ll need to “pinch myself” when I remember I can stay in my pajamas and enjoy another cup of coffee.
The treatment floor at SCCA is a series of individual treatment rooms with either a patient bed or chair set up for treatment. I estimate there are about 45 treatment bays scattered around the floor. I’m familiar with each hall and many of the bays as I’ve roamed this floor over the last 4 years (counting initial treatments). Today I was assigned bay 14. Just across the hall from bays 17 and 18. Those were the rooms in which I received high-dose chemo to kill my bone marrow and then received a transplant of my stem cells to reboot the production of healthy bone marrow. My autologous stem cell transplant (ASCT) happened here.
It probably snuck up on me, but suddently I put together the significance of reaching MRD negavtive status, dramatactily reducing my treatment regimine, having my doctor express how good I looked nearly five years from the first time he saw me. I am working nearly as much and as hard as I did the day before my diagnosis. I’m able to participate in nearly every past-time I’ve enjoyed my entire adult life. I have accomplished so much. Today there are so many objective and subjective measures telling me I have accomplished so much.
I have read in the past about other types of cancer patients getting to “ring a bell” as they leave their treatment for the last time. A sign of completion, joy, celebration. I’ve lamented at times that myeloma patients won’t ever “ring the bell” beacuase we never know when our treatments will be done. But walking down the hall on this day I mentally “rang a bell”, taking a last look around and silently saying “goodbye.”
Chances are this state is not permanent, but today I won’t think about that. Today is a truly remarkable day standing out at the beginning of many more remarkable days.
The sunrises on another day, another field, in the Skagit Valley farmlands. The fields have produced crops for decades, but each day brings a new sunrise, new hope, a future crop.
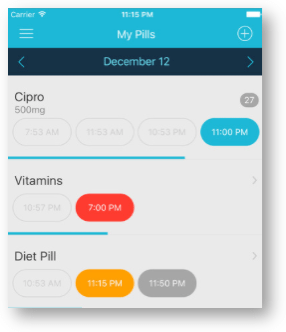
Product Review: Easy Pill – A quick and easy application to track the many daily medications I take.
Easy Pill screen shot.
Until my diagnosis, I didn’t regularly take any medications so tracking when to take a pill was never an issue. Of course, multiple myeloma changed all that. Since my stem cell transplant, I take about 11 pills per day. I say “about” because the number varies; I take at least five extra pills on infusion days, and I intermittently take additional medications to address insomnia, heartburn, cramping, neuropathy, pain, and other side effects.
Being a geek at heart I looked at this new reality as an opportunity to find a technological solution, hopefully one that involved my iPhone and AppleWatch.
I discovered an application called Easy Pill for iOS by BirdsCorp.com and have been using it since 2016. Easy Pill is an iOS app that tracks my medications and gives me reminders when it’s time to take a pill.
The obvious first step to using Easy Pill was to input my medications into the app. I could create a list of medications either on a mobile device or the Easy Pill web page.
I didn’t use the web page, but if I had, I would have created a list of all my medications, doses, and schedule. The page then creates a QR code to scan with the app which then transfers all the information into the app. I tested this method and it works well. At the time I started using the app, however, I didn’t want to upload my medications to a web page I hadn’t researched.
I chose, instead, to input my information directly into the app on the phone. I wouldn’t call this process “intuitive”, but it didn’t take long for me to get the hang of it.
Honestly, part of the challenge was a good thing because it comes from choosing between the many options available. How often do you take the pill? Do you take the pill the same time every day? What is the duration of time taking this pill? Easy Pill offers a lot of flexibility to tailor the schedule exactly the way I want it for each medication. It took me a while to get everything the way I wanted, but I appreciated that I could create a schedule that was accurate and useful.
Medications can be viewed in two different ways. In one view, pills are listed alphabetically with all their vital information. The more useful view, and the one I use most of the time, is the daily view. It shows a chronological list of all the pills I take each day. An icon next to each pill tells me the time to take the pill and the color of the icon gives a visual cue if a pill is overdue or needs to be taken in the future.
The most useful feature of Easy Pill is that it reminds me to take my medication. This is accomplished with simple alerts that appear on the phone and with a tap on my wrist from my watch. The app gives options for setting up the type and frequency of the reminders so the app can nag as much or as little as I like. When the pill is taken a single touch on the phone or watch logs the dose as taken.
Easy Pill records the exact time I took medication and the icon for the pill changes to alert me that the status has changed. I can also skip a dose or pause a medication from the reminder alert. When I finish a course of medication Easy Pill remembers that and automatically moves the medication to the archives. I can open the archives to look at the history of the medication, or move it back into my active schedule if I start taking the medication again.
I use the archives to reactivate the cycles of treatment. For instance, I take Pomalyst twenty-one of twenty-seven days. When I take pill twenty-one, the app moves Pomaylst to the archives. When I begin a new treatment a cycle I just change the start date on the archive listing and Pomalyst becomes active again in the day view on day one of the new cycle.
Another handy feature of Easy Pill, though I haven’t used it much, is a direct Google link for each medication. I can follow the link to find information about and images of each medication. This is a nice way to remember what a pill looks like and learn about common side-effects.
Easy Pill not only reminds me to take my medications, but it tracks my progress in a number of ways. Easy Pill reports how many doses and how consistently I took the medication. If I input the quantity of pills when I start, Easy Pill will remind me when it’s time to refill the prescription.
Easy Pill also exports a medication list that includes pills that are currently taken or archived, detailed medication information and a dose log. This could be useful when I need to share a complete history of all my medications with care providers.
Easy Pill is $2.99 and it works on the iPhone and iPad. Oh look, its time to take another pill… until next time.
Highly sensitive imaging can be performed to identify myeloma lurking inside and outside bone marrow.
As I wrote in my last column, I recently learned that I am MRD negative. There are a few different test methods to detect minimal residual disease and the prognostic value of the tests varies with the testing method employed.
In my case, after doctors withdrew a sample of bone marrow from my hip it was assessed using next-generation sequencing (NGS). As I understand the process, an older marrow sample is used to identify the DNA of my original myeloma cells. The assay then looks for that DNA sequence against millions of cells in the newly extracted marrow, in my case 2,922,325 cells. If no cells with matching DNA are detected there is no minimal residual disease and the patient is said to be MRD negative.
It is possible, however, that sequencing of the cells from a marrow sample may not detect all residual disease because myeloma can appear outside the marrow.
A PET/CT (Positron Emission Tomography)/(computerized tomography) scan is an imaging technology that allows doctors to “see” areas in the body where multiple myeloma has caused tumors in soft tissue and/or congregated in the marrow. While sensitive analysis of the bone marrow can detect MRD inside the marrow, a PET/CT can detect minimal residual disease inside and outside the marrow. This is called “imaging” MRD testing.
To perform a PET scan a radioactive sugar is injected by IV. The sugar travels in the body normally and creates a “tracer”. When the patient is scanned about an hour after injection, images of the distribution of the sugar are obtained. Because cancer cells use sugar at a higher rate than normal cells they appear as “hot spots” in the images. The PET scans are merged with the CT tomographic x-rays, cross-sectional images of anatomical structures, to show doctors with great specificity the existence and location of cancer cells.
It is well accepted that patients that achieve a deeper response to treatment are more likely to enjoy longer progression-free and overall survival. So it follows, achieving MRD negativity, the deepest response that can currently be measured, is a good prognostic predictor. While it seems logical, research last fall concluded that patients that are both MRD negative in a bone marrow assay and imaging analysis have statistically improved progression-free and overall survival.
The PET/CT is an interesting test, but generally not too uncomfortable unless you are claustrophobic or have trouble being still for long periods.
To start, I began fasting six hours before the test and couldn’t exercise in any way. Exercise “fires” up the muscles and changes the way the muscles metabolize sugars, and that would throw off the scans. Presumably eating causes a similar issue. The fasting was a challenge, but I didn’t have much trouble sitting idle all morning and watching television.
When my appointment began I was injected by IV with a radioactive glucose solution. I didn’t feel anything, but I was suspicious when the nurse pushed herself away from me as we continued our small talk. When the injection was complete I was told to relax and not move around for forty-five minutes to let the tracer fluid distribute through my body. I heard “take a nap” and I always follow directions.
I was called back to the scanning room and directed to go empty my bladder as best as possible. “Be careful not to get urine on your hands, it’s radioactive. Wash up well when you are done.” Encouraging instructions, I’m sure this is all safe.
Lying flat on my back, my head in a U-shaped pillow, the bundling process began. A large rubber strap was placed around both arms at my biceps, the weight of my arms against the strap holding them in place at the sides of my chest. My toes were similarly bound to keep my feet and my legs from rotating outward. Having my arms and legs thoroughly secured, I was swaddled head-to-toe in warm blankets. This was welcome as the room was frigid.
Now resembling a mummy, the slab I was on moved back and forth, foot to head, through the large round scanning machine. It’s a bit like being passed through the hole of a giant donut.
Before the scan started the technician explained the procedure and emphasized that if I moved we would need to start over. The scanning process was easy. I tried to relax as best I could, listened to the music in the room, and tried to ignore the desire to move around. Of course, as we started I experienced an uncontrollable urge to cough. Thankfully, about 30 minutes after we started the scans I was informed they were complete and “useable.”
I was sent home to await the results. Unlike the cellular assay, when I expected the tests to detect at least some minimal residual disease, I hoped the PET/CT would confirm the earlier MRD negative findings. The PET/CT found “No abnormal osseous or extraosseous radiotracer uptake to suggest viable myelomatous involvement.”
In other words, the doctors were unable to identify any minimal residual disease in either the assay or imaging. Time to take a breath and savor another victory in this long journey.
“Morning Calm” was 0ne of the first photos I captured when I recognized something special and needed to share it with others. The photo was taken very early in the morning on North Twin Lake. “Mirror” images are a common tool for photographers, showing the real and the reflected. By capturing a moment in time we get to see what the eye sees naturally as well as a fleeting hidden image seen only when the waters are calm.
Living with multiple myeloma is full of ups and downs, twists and turns and surprises. For me an unexpected twist has led to a very happy place.
Welcome ladies and gentlemen to one of the scariest rides of our generation. It will bring you to the highest point only to drop you down at unimaginable speeds. You will enter turns you never see coming and remain breathless to the very end. Welcome to the multiple myeloma roller coaster.
When last we spoke, I was celebrating three years post-ASCT and preparing to pare back my aggressive 3-drug maintenance regimen to something more manageable. I looked forward to a return of precious time to me and my family. Since that column, the plan shifted to more testing and continuation of the same treatment regimen.
The good news is that my general health remains outstanding with no apparent changes in my myeloma. Regular blood tests continue to register no measurable monoclonal proteins, my free-light chains are normal, and my other blood counts and kidney functions are good for a person taking regular chemotherapy medication.
My physical health is strong, in fact, we ended the summer with a fabulous family vacation to New York and I wrapped up the year attending two-week-long conferences in Minnesota and Tulsa with several hundred colleagues.
Shortly after writing my last column I met with my doctor, but the conversation didn’t go as I expected. Instead of suggesting a reduction in treatment, he said he wanted to continue the three-drug regimen indefinitely. The reasoning was understandable, given my high-risk cytogenetics, but it was still a big disappointment.
Approaching this meeting I felt I’d achieved an unexpected turning point in my myeloma journey. The treatments had gone so well that I was considering an even greater return to my pre-diagnosis life. While that was always my hope, I didn’t know if it would happen and reaching that point was cause for celebration. While not intended, the conversation with my doctor tempered the celebration. Wrongly or not I felt a level of defeat.
More realistically, it all comes down to the risk of relapse. All myeloma patients have the same goals; find the best method to forestall a relapse as long as possible, and be prepared for a relapse of myeloma that is more difficult to fight than the prior incarnation. For high-risk patients like myself, the goals are the same, but the chances of a harsh relapse are greater.
My current treatment has achieved complete response for a substantial time and there are no current signs that is about to change. I’ve tolerated this level of treatment extremely well. The theory, as I’ve been told, is “if what you are doing is working keep doing it, otherwise do something else.” Because the disease could return more aggressively and may not respond as well to the next treatment there is great value to preserve the progress I’m enjoying today for as long as possible.
My doctors and I both recognized we needed more information to make this decision. On my doctor’s advice I underwent another bone marrow biopsy in November 2019, but this time we would test for minimal residual disease (MRD). With a regular blood test, doctors can identify one cancer cell in up to one-hundred thousand blood cells. By contrast, MRD testing can identify one cancer cell in one million blood cells. Because it requires a bone marrow biopsy and it is more costly than blood testing, MRD testing is not regularly prescribed. Myeloma professionals also still debate the value of MRD testing as it relates to treatment decisions for individual patients.
Because the testing requires such precise measurements I waited sixty days for the results. I was not expecting that length of uncertainty, but I tried to temper my expectations. Given the current science, being MRD negative, finding no minimal residual disease, is still fairly rare and a bit of a milestone. During my wait, I assumed I was MRD positive (there must be a monoclonal cell hiding somewhere). I felt it was better to expect the “worst” and be surprised by the best.
I finally received my MRD test results on January 15, 2020 (a whole decade after the procedure). I was shocked and ecstatic to learn I am MRD Negative.
My first reaction was surprise. Perhaps because I’ve conditioned myself to be hopeful, but not overly optimistic I didn’t expect this result. My second response was to feel validated. At least that’s the word that comes to mind. I’ve felt healthy and “normal” for a long time, but knowing I had multiple myeloma and all that goes with it I figured it was a bit illusional. While I know MRD Negative doesn’t reflect any sort of “cure”, and I remain vulnerable to relapse and all the attendant risks of myeloma, at least for this moment there is no myeloma. I’m feeling healthy because there is no cancer. I’m not fooling myself, I deserve to feel good.
I have a new appointment to have a new conversation with my doctor. We may decide that some level of treatment will continue, but I won’t be disappointed this time. I have proof that all the work and effort is paying off. I have cause for celebration, but I’m not letting down my guard.
A lesson learned from my myeloma journey is to not allow myself to get too high or too low. Since my diagnosis I’ve been up and down the roller coaster enough times to prepare for the next big turn or drop. For now my arms are raised high, I have a big smile on my face and I’m ready for whatever comes next.
────────────── ♦ ────────────────
Photo Credit: (c) 2019 Mark Pouley.
My family closed out 2019 making a trip to New York. For a week I set aside being a myeloma patient as we went all-in as tourists enjoying all the sights, sounds, and tastes of the “Big Apple.”
Celebrating the three-year anniversary of my stem cell transplant brings new choices about treatments and the possible improvement in my quality of life.
Today, however, I’m still enjoying a complete response and relatively good health with remarkably few side effects. My perspective on the future also is much brighter, and three more years of good health doesn’t seem like a stretch anymore.
Much of my current success is due, I believe, to the aggressive maintenance treatment I have been receiving. This third anniversary is not only cause for celebration of 36 months of progression-free survival, but it also raises a decision about how to proceed.
A quick review of my history lays the groundwork for the decision I face this fall. I was diagnosed in 2015 with “high-risk” multiple myeloma due to the presence of the del(17p) chromosomal abnormality. I was initially treated with Velcade (bortezomib), Revlimid (lenalidomide), and dexamethasone, which proved ineffective. I moved on to Kyprolis (carfilzomib), Pomalyst (pomalidomide), and dex (KPD), followed by an autologous stem cell transplant. At 60 days post-transplant, I had achieved a nearly complete response and had to decide whether and what maintenance therapy to undergo.
July 22 marked the third anniversary of my autologous (own) stem cell transplant. Honestly, although the treatment went well, when I was sent home, three-years in the future seemed like a very long time away. I wouldn’t have been surprised if a relapse had arrived before this day.
If I’ve learned one thing about multiple myeloma, it’s that it can be uniquely personal in the way it develops and affects a patient, but more so, how it will react to treatments. Maintenance therapy, it seems to me, can be even more of a gamble then initial treatments. If a patient responds well to initial treatment and a transplant, is there a reason to continue treatment to maintain that progress? This can be a tricky question, especially for standard-risk patients who did well after initial treatment. In a nutshell, all treatments come with risks. To undergo maintenance therapy, a patient must decide that the chance of achieving extended progression-free and possibly overall survival outweighs those risks.
There is data suggesting that maintenance therapy for “high-risk” patients like me can extend time without relapse, so following my transplant, my doctors recommended an aggressive maintenance therapy of a half-dose of the previous KPD treatment. This decision was based on research out of Baylor University that supported a triplet of medications for three years for high-risk patients.
During the first ten months after my transplant, my lab results showed a barely measurable amount of M-protein. After that, over two years now, there has been no measurable amount of cancer detected in my blood tests. By all standards, this is a great result and consistent with the best outcomes reported in the Baylor study. While there is no way to know if my current condition is because of the maintenance treatment, given all that has occurred in the last three years, I believe the decision to proceed with the aggressive maintenance therapy was correct.
Now that I’m approaching that three-year mark, I must decide what’s next. It’s easy to think that if the disease is being kept at bay and I’m not suffering many side effects, I shouldn’t change anything. Though my current results are all we could have hoped for, as I understand the research, there is little information about what benefits, if any, I might achieve by continuing this treatment beyond three years. There is, however, an ever-growing risk that the toxicity of the treatments will eventually be more than my body can handle, and that may open the door for more serious side effects or secondary cancers.
Since there is a lack of clear data about the clinical benefits of continuing this aggressive course of maintenance, I will decide based primarily on how the treatments impact my quality of life.
I’m convinced that Kyprolis is a myeloma-killing champion for me. Other than my transplant, it also has had the most significant impact on my quality of life. Kyprolis is administered by infusion. As an initial treatment, it required trips to the clinic on two consecutive days three weeks on, one week off. As maintenance treatment, the trips are cut to one day a week, but still three on, one off. For me, that means a two-hour roundtrip drive and anywhere from two to five hours at the clinic. Since starting Kyprolis in January 2016, that has been a lot of time on the road and in the clinic. Since my appointments are generally Friday or Saturday, it also means I can’t plan to travel or participate in an activity on many weekends because I have treatment.
My wife and I cope with this schedule because we understand it is necessary and because my getting better has become one of our jobs. We are used to the inconvenience in our schedules and our lives, but it would mean everything to retake this time from the disease.
Time, I have discovered, is more precious to me than anything else. Time with my family. Time with my grandchildren. Time to take pictures and enjoy the world I live in. Time to work on the projects that are priorities to me at work. Time is finite with our without myeloma, and making use of the time doing what I want to do, instead of sitting in traffic or in a clinic bed, is the ultimate improvement to my quality of life.
Based on the ever-increasing risk of toxicity, the lack of compelling evidence I would improve my chances of long-term survival, and the thought of even a short-term return to a more normal life, I have decided to drop the Kyprolis from my on-going treatment plan. On my doctor’s advice, I will continue the oral medications of Pomalyst and the dreaded dexamethasone. We will closely monitor my health and meet regularly with my specialist, ready to change course at the first sign of a relapse.
When I was first diagnosed, I looked at treatment as a way to avoid dying. On this anniversary, I celebrate the past success and look at maintenance therapy as a way to keep living my life.
────────────── ♦ ────────────────
Photo Credit: (c) 2019 Mark Pouley
I celebrated my anniversary this year, as in the past, vacationing at our eastern Washington lake retreat. As always, it was splendid. When we’re at the lake, I spend early mornings on my boat looking for scenery and wildlife to photograph. This year a bald eagle let me get unusually close, and it stayed and posed for many great photos.
The unexpected passing of my cousin has me thinking about life and death and the memories we leave behind when we’re no longer here.
Just before Thanksgiving, I received word that my cousin John passed away. His memorial was held the Saturday following the holiday. There isn’t anything that makes me think about life and death more than the passing of a friend or relative (except perhaps my cancer diagnosis). The fact it happened during a time when I was with nearly all of my family made it that much more significant.
I hadn’t seen John in about six years, and we spent no time together as adults. Still, the news of his death hit me hard. In part, it was the sudden and unexpected nature of his passing from a heart attack, but more so that our shared childhood adventures are so much of my past, and now he is gone.
It’s not a stretch to say that I grew up at John’s house. When my parents left town on occasion, I would stay with John and his sisters. When I wanted to have a fun weekend, I would ask my parents to let me go to John’s. My aunt and uncle were great substitute parents, and John had all the cool toys my parents wouldn’t let me have: motorcycles and BB guns. He lived on acreage in a rural setting, and we spent many hours exploring and playing on the open land and in the irrigation canals.
Thinking about John’s passing, I realize that John and those adventures are all part of my most memorable childhood stories, the kind you tell your own kids decades later when you want to share what Dad was like as a kid.
A couple of the stories I’ve shared many times with family and friends stand out.
Once when I was young, my parents took me to John’s to spend the weekend. They were never fans of motorcycles, but when they dropped me off, I was expressly instructed to stay off the devil machines. Of course, John and I rode his dirt bike that weekend. It wasn’t enough, though, to ride the motorcycles. John was going to teach me how to jump the bike out of the dry irrigation canals.
The idea is simple enough: drive down one side of the ditch and up the next, “catching air” as you escape the ditch. John did it like a pro. His riding skills surpassed mine by a lot. On my first attempt, I rolled down into the ditch and throttled the bike up the other side. Unfortunately, I failed to maneuver the short distance between the canal and the barbed-wire fence running along the canal. My failure is chronicled to this day by the scar on my right cheek where 36 stitches closed the gash torn in my skin by the fence.
In one of the outbuildings at John’s, there were several animal traps hanging on the wall. John told me that they were his and that he used them to trap muskrats in the canals. From that moment, I wanted to trap muskrats. One winter weekend, we finally got the chance to set John’s traps along the canal. When we checked them later, we found a muskrat trapped by the leg, but still alive. John handed me the bat he’d been carrying, offering me the honor of the kill. The muskrat looked at me with sad muskrat eyes and I couldn’t do it. It’s really a wonder I’m not a vegetarian today, but I will never forget that moment.
These are my stories. At John’s memorial, friends, family, and co-workers shared story after story about John. It was a really special tribute to a great guy.
John’s memorial reminded me that we are our memories and the memories held by others.
John left us suddenly and without warning. I haven’t spent significant time with him in almost 40 years. Even so, he lives after his passing in my vivid memories and the many, many stories shared by others at his memorial.
When I look back on my childhood, who I was, and the things that influenced me, I remember those stories and so many more that live on in me all these years later. Those adventures shape who I am today.
My wife often says it is our job as parents to make memories for our kids. Taking them to Disneyland, sharing family traditions, showing them the world we live in, is all about helping them make memories. I know we’ve done a good job of this with our children, and now I’m working on making memories with our grandchildren. I hope when they are my age they will smile when they think about their crazy Papa.
As long as we’ve been married, my wife and I have hosted Thanksgiving in our home. When we were in school, we invited friends who couldn’t get home to their families. Today, our entire family and many significant others join us for a day of fun and food that often spills over through the weekend. It’s been so many years that the traditions and stories of past Thanksgivings are etched in the everlasting memories of everyone. It is a highlight of our year, and a highlight of my life. Each year the traditions are the same, but each year is different, and we build on the memories of the past.
There is a 100 percent chance I will leave this existence, regardless of multiple myeloma. It is also a certainty that family and friends will remain here and go on without me. If I’m lucky, and I believe I’m very blessed, I will continue to live in their memories.
My family, my children, my grandchildren will celebrate Thanksgiving after I’m gone. It is possible the location will change over time. The people able to attend may also change. Still, many of the traditions will continue. The stories of our past holidays will be told with joy and laughter.
Each day it is our responsibility to keep the memories of those who have gone before us alive. It is our responsibility to imbue memories of ourselves in those we contact. John’s memorial service reminded me that we get to choose the nature of those memories.
We are our memories and the memories held by others.
────────────── ♦ ────────────────
Photo Credit: (c) 2010 Mark Pouley
An aesthetically pleasing landscape photo is good, but a really good image should tell a story. In some rare cases, a photo can also stir deep emotional feelings, at least for some of the people viewing it. For me and my family, this is such an image. This is the very first view of the Twin Lakes we see as we drive down the mountain road into the Inchelium area. This familiar glimpse of the water means our long trip is nearly done, and we are about to enjoy the pleasures of the lake, the outdoors, and the people.
Every cancer patient is bombarded with statistics about survival rates, and “high risk” patients get the short end of those statistics. Instead of giving those numbers too much power, we need to remember what’s really behind them and how they apply to an individual patient.
I was recently reminded of an important lesson about statistics that applies to multiple myeloma. Interestingly enough, I was reminded of the lesson sitting in a stadium full of soccer fans, of all places. While a regulation soccer match is 90 minutes long, the official time is kept by the referee and he or she can add a few minutes to every match to compensate for the time play was stopped for injuries or other reasons. In the 93rd minute of the last game of the regular season, the Seattle Sounders scored a goal that shattered statistics.
The regular season of Major League Soccer (MLS) starts in early March and ends in late October. Like many American sports, the regular season is followed by a playoff to declare the final champion. The Sounders won the championship in 2016 and played in the championship match, but lost, in 2017. The Sounders have advanced to the playoffs all 10 years they’ve been in the league, but in 2018 it appeared this streak would come to an end.
When the 2018 season began, the team’s star forward suffered a season-ending injury in the first match. Clint Dempsey, arguably the greatest American soccer player ever, retired mid-season after barely getting on the pitch in 2018. Losses piled up early. Some close games were given away, some matches weren’t even close. It seemed the season was lost before it really got going.
There are several organizations that compile sports statistics that track soccer teams’ successes, and failures, game-to-game. The numbers are used to project a team’s likely finishing position. In June, about mid-season, the Sounders had the worst record of 23 teams and were given only a 1.67 percent chance of making the playoffs in 2018. From my vantage point, that number seemed generous. The team looked terrible.
Many loyal fans, even in my household, wrote off the season. All objective information before us suggested the team was going to finish the season outside of the playoffs. It wasn’t a matter of giving up hope; looking at all the facts, this seemed like the only reasonable conclusion.
In July, the Sounders started winning matches, and by the end of October, they turned in the best half-season of soccer in MLS history. They not only qualified for the playoffs, but with the goal scored in the dying minutes of the last game of the season, they finished with the fourth-best record in the league.
The Sounder’s playoff games begin on November 4 (likely before this column is published). The statisticians give the Sounders only a 9 percent chance of winning the championship. Given what I learned this year, I’ve decided to ignore the numbers and just enjoy the games.
As myeloma patients, we’ve become pretty familiar with statistics. There are numbers everywhere we look. Every treatment comes with a spread of numbers suggesting how many patients might respond to a given treatment, how likely the response will be complete and whether or not the treatment might, in comparison to other treatments, extend a patient’s progression-free and overall survivals. Of course, we are all familiar with some of the grim statistics regarding the number of months or years a myeloma patient might expect to live, regardless of treatment. As I’ve discussed in other columns, I’m considered a “high-risk” patient, and the statistics for the group of patients that share my chromosomal abnormality are not very cheery.
Cancer patients are often warned against giving too much stock to statistics, and for good reason. The statistics we see are merely summaries of a collection of data from a set of patients within a given category. Even within the measured collection, some patients did better and some patients did worse than the final averages and medians. There are numerous factors that influence how relevant any given data might be to our own particular case. As a single example, when discussing the overall survival of myeloma patients, one factor that can skew life expectancy statistics is the vast number of treatments that have been introduced in the last 10 years.
I’m not questioning the accuracy or validity of statistics. Statistics are critically important to researchers and doctors that are making long-term decisions about caring for myeloma patients. Statistics are especially important to draw general conclusions about a set of data from a sample. The numbers we see today are encouraging for the future of today’s patients and those who follow us. There is a reason for hope for all patients, but that too is a generalization.
For individual patients, and for me in particular, how well a specific drug worked on average for a group of patients studied in a particular location during a window of time is far from a perfect prediction of how well I’ll respond to the drug. How long the average myeloma patient diagnosed in 2010 survived does not tell me whether I’m likely to to watch the 2022 World Cup or not. How well I do in treatment, how long I will survive, is controlled by too many factors, knowable and not, to make any reliable predictions.
During the post-game press conference following the last match of the regular season, the Sounder’s coach was asked if, given where the team was in June, he honestly believed his team would make the 2018 playoffs. He gave a wry smile and quickly responded yes because he knew the team had it in them to turn the season around and beat the odds. The people forecasting the Sounder’s final position in the league weren’t wrong, they just didn’t account for the many individual factors that influenced the outcome of the season.
The survival numbers and treatment reviews aren’t wrong as they relate to the myeloma population overall, but they are much less relevant to any single patient. There are just so many factors that skew the numbers one way or the other. In some areas, I’ve already surpassed the averages for “patients like me.” In other respects, I’ve still to reach some longer milestones.
From my perspective, the lesson of the Sounders’ 2018 season is that for each individual person, none of the numbers really matter. I will do everything in my control to stay as healthy as possible. My care team will apply all methods possible to keep me healthy. I will get exactly as much time as all the factors taken together will deliver to me. Each day I’m here, though, I will sit back and enjoy the game.
UPDATE (November 9, 2018) – Unfortunately, the Sounders were eliminated from the playoffs on November 8 by their hated rivals, the Portland Timbers. Just as they had during the regular season, the Sounders played to the very end, including thirty minutes of overtime and penalty kicks to break a tie. Objective observers are calling it one of the greatest MLS playoff matches ever. The Sounders entered the match with long odds of advancing, and through multiple dramatic lead changes met the challenge and pushed the opportunity to advance to its limit.
────────────── ♦ ────────────────
Photo Credit: (c) 2013 Mark Pouley
Centurylink Field, home to the Seattle Sounders FC (and the Seattle Seahawks) is one of the most beautiful pitches in the MLS. On many days, like this one in 2014, the view is magical. During the last 10 years I’ve found refuge from a busy life in the stands, but since my diagnosis, attending games has taken on a very special meaning and given me great joy.
Maintenance therapy for multiple myeloma can feel a bit like treading water. My disease is in check, but I’m just paddling about to keep my head above water. But sometimes treading water is a good thing.
As I enter my third year of maintenance therapy after experiencing very little change in my health the past couple years, I sometimes feel as though I’m just “treading water.”
While it’s often considered derogatory to say that someone is treading water, being able to swim in that way is actually a very important safety skill. A swimmer isn’t going to make any forward progress treading water, but they’re going to keep their head above water (i.e., not drown) long enough to catch their breath so they can continue a longer swim. Treading water also allows a person who gets stranded too far from shore to survive on their own while waiting for help to arrive.
When I was diagnosed with multiple myeloma, the purpose of initial treatment, and the measures of its success, were obvious. The same holds for the stem cell transplant that followed my induction therapy. In those instances, the energy and resources expended on treatment, and the toll the treatments took on my body, moved me forward by significantly reducing the number cancerous cells in my body.
The purpose and measures of success for maintenance therapy aren’t so obvious.
This is true not only for patients like me, who have no medical training. Maintenance also is a subject of discussion even among myeloma specialists. While maintenance is generally recommended by doctors in the United States, it remains unclear what its actual benefit is in terms of a patient’s overall survival. This allows doctors and patients to question the value and necessity of recommending maintenance therapy for all myeloma patients.
Just as there are many types of initial treatment available for multiple myeloma, there are a variety of options when tailoring maintenance theray to individual patient needs. It is truly remarkable that multiple myeloma patients have so many treatment choices available. It does, however, make it more difficult to decide what course of action to take because it often seems whatever path we choose may foreclose other options.
Whether to proceed with maintenance, and what type of maintenance to pursue, are particularly difficult decisions because the benefits seem so hard to quantify, and there is a natural desire to be free of treatment, even for a short period. If I simply think of maintenance as holding the status quo, it can seem like a waste of energy. However, when I understand the true importance of “treading water,” the case for maintenance therapy seems to me to be more compelling.
The main argument in favor of maintenance therapy is that studies consistently find it extends the remission patients experience while they are undergoing maintenance. The treatment reduces any residual disease that exists in patients and delays the time until the residual disease begins to multiply, causing relapse.
The costs of the treatment, aside from the financial expense, are the side effects and other possible harm caused by the long-term toxicity of the treatment. For me, the price includes the hours of driving to and from the infusion clinic three weeks per month; taking a handful of pills daily; and suffering the constant fatigue and occasional cognitive lapses. There also are real health risks associated with long-term maintenance, such as secondary cancers or heart damage, which can decrease rather than increase overall survival.
All this simply to stay in place.
I’m treading water with no movement forward. Or so it seems. If maintenance treatment doesn’t extend my overall survival, is there enough reason to endure the possible toxicity of treatment?
The problem, both from the scientific perspective and the patient’s perspective, is that it is so difficult to know with any certainty if the treatment is extending an individual patient’s survival. While some studies support this conclusion as a general proposition, as an individual it isn’t possible to know if the medications are effective or not.
If I don’t relapse, is it because I’m undergoing maintenance treatments? Might I also avoid relapse if I stop treatment? If I take a “drug holiday,” could I avoid relapse and the fatigue, neuropathy, and other side effects of the medications?
There is no way to answer these questions, so I have to decide if it is worth the risk of relapse to stop treatments.
Given the relatively mild side effects I’m experiencing and the fact that my high-risk myeloma remains at bay, I’ve decided, with the support of my myeloma specialist, that the benefits of maintenance outweigh the cost.
I am hopeful that a relapse is very far in the future. Realistically, though, I must prepare for the possibility that it is just around the next bend. I need to be fully prepared for that and the toll it will take on me to deal with it. Like the swimmer treading water, right now I’m just resting, keeping myself healthy enough to be ready for another tough swim in the future.
I’m convinced that my current maintenance treatment gives me my best chance at sustaining this progression-free period of my life. That is important for many obvious reasons, but given my relatively young age and my commitments to my career and family, I want to spend this time with my head above water.
────────────── ♦ ────────────────
Photo Credit: (c) 2014 Mark Pouley
A duck calmly sits on a log at the crest of Niagara Falls as the roaring water rushes by. This photo reminds me how important it is to be content holding on in one place while everything around me moves by quickly.